HEADACHES ( THE BRAIN’S EQUILIBRIUM )
HEADACHES In the waning days of the Civil War, Union general Ulysses S. Grant was suffering from a terrible headache. He stopped at a farmhouse in the rear of his army, which had been pressing the forces of Confederate general Robert E. Lee. “I spent the night in bathing my feet in hot water and mustard, and putting mustard plasters on my wrists and the back part of my neck, hoping to be cured by morning,” Grant wrote in his journal on April 9, 1865.
Shortly afterward, Grant was visited by a messenger who carried a note saying Lee, who had refused to surrender the previous day, had changed his mind and would be willing to meet to discuss a formal end of hostilities. “When the officer reached me,” Grant said, “I was still suffering from the sick headache; but the instant I saw the contents of the note I was cured.”

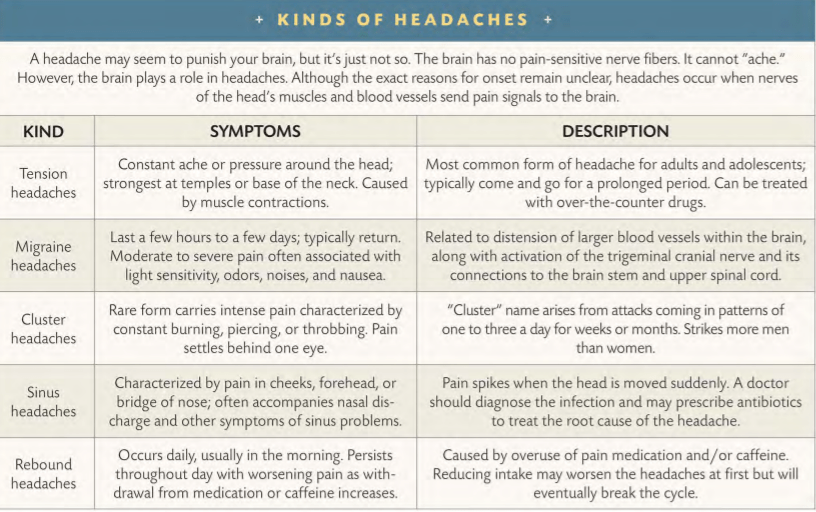
Grant probably suffered from a muscle-contraction, or “tension,” headache. Typically, a tension headache begins when the neck, scalp, and face muscles are tensely held stiff for a long time. The most usual source is prolonged anxiety, a debilitating form of stress. Grant needed Lee to surrender; Lee’s announcement of his plans took the worries, and the agony, away. “The pain in my head seemed to leave me the moment I got Lee’s letter,” Grant reportedly told an aide as he rode off to end the war.
HEADACHES CATEGORIES
Even as it serves as an indicator that homeostasis is being disrupted, a headache is not a disease per se. Instead, it maya symptom of some other problem. It can manifest itself in response to irritation of blood vessels in the head, or to an injury or imbalance, or to inflammation of bodily tissues, to disorders related to stress-or to a host of other possible triggers. While it may feel as if the brain screams in pain, a headache can only occur outside the brain itself, which contains no pain receptors.
Headaches come in dozens of varieties. An easy way to categorize them is by the ways they cause pain. Muscle contractions such as Grant’s are one of the most common sources, especially among those living with high levels of stress. Dilation of blood vessels is a second typical cause. When arteries expand in the head, they squeeze against surrounding tissues, producing viselike pressure and pain. Fever, migraines, drug reactions, changes in blood pressure, and carbon dioxide poisoning can provoke dilation. Internal traction an abnormal growth in the head, for example is a third trigger. When a tumor presses against other tissues, or the brain itself begins to swell, the pressure causes pain. Inflammation is a fourth common source. Allergic reactions and infections such as meningitis can irritate pain-sensitive receptors in the head. Finally, headaches can occur without an obvious physical cause. These headaches are called psychogenic, meaning they arise in the psyche. They may spring from an emotional problem, as the sufferer converts emotional pain into real, physical symptoms.
The word migraine evolved from the Greek word hemikrania, meaning “half-skull.”
Many of these disorders strike not next to the brain, but in the eyes, sinuses, and other facial organs and tissues. Cranial nerves intimately connect the face and neck muscles to the brain, so it is no wonder pain sensations can spread until they feel as if they overwhelm the entire head.
Treating chronic headaches requires a proper diagnosis. Given the wide range of headaches and their causes, as well as the possibility of triggers working in combination, medical treatment often relies on detective work. At least, however, the efficacy of treatment has advanced since humanity first tried to cure a headache. A thousand years ago, Arabs recommended applying hot irons to the head, while a French medical treatise written in Latin urged sufferers to mix the brain of a vulture with oil and shove it up the nose. Today, modern pharmaceuticals, relax- ation techniques, and proper diet target dilation, tension, and other causes. One of the most effective pain relievers is common aspirin.

![GOOD FEELINGS / PLEASURE CENTERS [ THE NERVOUS SYSTEM ]](https://humanityuapd.com/wp-content/uploads/2022/10/Screenshot_2022-10-31-15-30-10-044_com.google.android.apps_.docs4_.png)

![PATHWAYS / GRAY MATTER [ MESSENGERS ( THE NERVOUS SYSTEM ) ]](https://humanityuapd.com/wp-content/uploads/2022/10/Screenshot_2022-10-29-15-14-24-029_com.google.android.apps_.docs_.jpg)

